
{kind=link}
✅ Ocular HTN or glaucoma suspect :
a patient with IOP above normal range (11 -21 mmHg) without any reported VF or optic disc changes characteristic for glaucoma
✅ To cut it short in points in treat ocular HTN and glaucoma suspect or not to treat:
We have to consider and evaluate the following risk factors when dealing with Ocular HTN or glaucoma suspect
✍️ Age
✍️ CCT( central corneal thickness)
✍️ IOP
✍️ CDR (cup/disc ratio)
✍️ PSD ( Pattern standard deviation)
✍️ Presence of DM or not
☝️ According to such risk factors we use online glaucoma risk calculator to get the presumed risk of developing glaucoma in such patients
☝️ If GRF ( glaucoma risk factors) value exceeds 15% you should start treatment with the least dose and frequency required to obtain satisfactory IOP reduction)

✅ In other words from treat ocular HTN and glaucoma suspect or not to treat:
Who to treat?!!
✍️ Isolated OHT: if IOP >27mmhg.
✍️ OHT and suspicious disc: if IOP >21 mmhg.
✍️ OHT and thin cornea: if IOP >21 mmhg.
✍️ OHT and only eye.
✍️ OHT and CRVO or AION in either eye.
✍️ OHT and FH of glaucoma (especially of blinding disease)
✅ relatively thin corneas (CCT <555 microns) were associated with a 3-fold risk of conversion to POAG versus thick corneas (>588 microns).
✅ Some practitioners use pachymeter routinely to correct the IOP for corneal thickness.
✅ One can roughly estimate for every 20 microns that the CCT is >550 microns, the IOP is under-read by 1 mmhg
✅ interestingly, this calculation reclassifies many NTG patients as high-tension POAG and OHT patients as normals.
Ocular HTN and glaucoma suspect treat or not to treat powerpoint presentations :
Glaucoma suspect,ocular hypertension, steroid induced glaucoma
- SCREENING AND EARLY DETECTION Comprehensive Eye Examination IOP – Pachymetry – Thinner CCT is a strong risk factor for COAG Slitlamp Examination and Gonioscopy Fundus Examination Skilled Optic Nerve Evaluation- HRT, OCT, GDx – ON Head and RNFL Standard automated Perimetry (SAP) Short Wavelength Automated Perimetry(SWAP) Ocular Blood Flow : Reduced Blow Flow in GS in the course of COAG. (Superotemporal rim-16%, cup -35% and inferotemporal rim – 22%).
- RISK FACTORS •IOP > 30 mmHg. •Thin CCT •Vertical C/D > 0.7 •Older Age •Abnormal VF : Increased Pattern Deviation •Presence of exfoliation or Pigment Dispersion Syndrome •Disc Hemorrhage •Family History •Fellow eye of patient with severe unilateral glaucoma •Additional – suspicious disc appearance, myopia, Low ON perfusion pressure, Steroid user, African Ancestor, sleep apnea, DM, Hypertension, CVS disease, Hypothyroidism, Migraine headache, vasospasm.
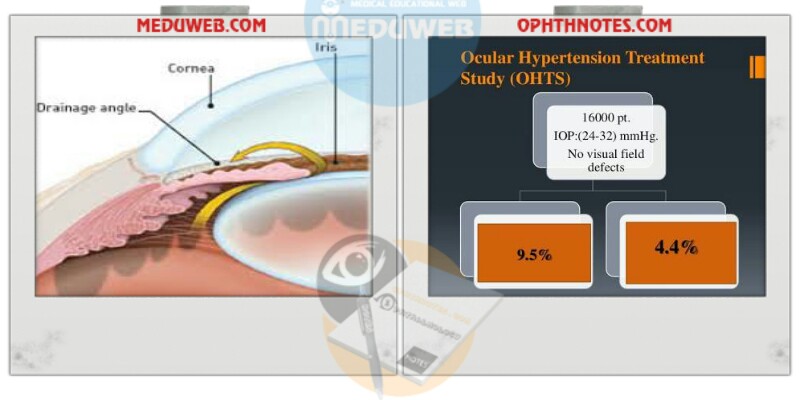
- RISK CALCULATORS Ocular hypertension treatment study European Glaucoma Prevention Society Diagnostics Innovations in Glaucoma Study
- WHEN TO TREAT Every attempt should be made to engage the patient in decision-making process. Elevated IOP should be stratified into low, moderate and high risk for progression. Patients at high risk for progression warrant treatment to prevent Optic nerve damage, whereas low risk should should be observed at periodic intervals. Moderate can initiate treatment if appropriate, or monitor closely. CAREFUL CONSIDERATION : Greater age and life expectancy Psychological factors Convictions Social environment Follow-up availability Pregnancy.
Ocular HTN and glaucoma suspect treat or not to treat videos :
(Ocular Hypertension and Glaucoma Suspects (OHTS) video