

{kind=link}
Pearls in Steroid Induced ocular HTN
✍ steroids change the TM ability to process aqueous due Glycoaminoglycan accumulation
✍ Alteration of TM endothelium phagocytotic ability
✍ Prevent release of enzymes that normally depolymerize GAGs
✍ Topical or oral corticosteroids can cause IOP rise
✍ Ointment or creams periorbital and inhaled steroids can cause IOP increase
✍ May be seen in patients endogenously producing excess steroids (e.g., Cushing’s syndrome)
✍ 2 -5 weeks onset (often longer) to develop
✍ About 2/3 of population are steroid responders
✍ only 10% of steroid responders have significant problems
✍ Response is dependent upon
• Frequency
• Dose
• Genetic predisposition : TIGR/Myocillin gene( AR inheritance pattern).
High risk patients in Pearls in Steroid Induced ocular HTN:
✍ Myopes
✍ Pts with POAG
✍ Children ( most dramatic response)
Treatment in Pearls in Steroid Induced ocular HTN:
✍ medication cessation
✍ Aqueous suppressants( beta blockers, CAIs,..)
✍ Prostaglandins
✍ ALT or SLT (poor prognosis )
✍ Trabeculectomy with or without antimetabolites.
Pearls in Steroid Induced ocular HTN Powerpoint Presentation:
- Definition Steroid-induced glaucoma is a form of secondary open angle glaucoma that results from the use of steroids.
- Epidemiology 5 to 6 % of the healthy subjects will develop marked elevation of IOP, 4 to 6 weeks after administration of topical dexamethasone or betamethasone eye drops. directly related to the frequency and duration of usage. The risk factors include preexisting primary open-angle glaucoma, a family history of glaucoma, high myopia, diabetes mellitus and young age.
- Epidemiology( continue… ) Greater Risk with Strong steroids (dexamethasone, prednisolone… ) Lesser risk with weak steroids (Rimexolone, hydrocortisone … ) Greater risk with ocular route ( topical, periorbital and intraocular ) Lesser risk with extra ocular route ( systemic and local )
- Pathophysiology Exact pathophysiology is unknown. But its known that IOP is elevated secondary due to increased outflow resistance of aqueous humor due to the accumulation of these substance and blockage of the aqueous outflow. 1. Increase accumulation of glycosaminoglycan’s. 2. Increase collagen, elastin and fibronectin. 3. Steroids also suppress phagocytic activity.
- Sign & symptoms With steroid-induced glaucoma, the pressure elevation is gradual. Therefore, like primary open- angle glaucoma, very few symptoms exist like: IOP increase, cupping of disc, nasal field defect, scotoma, blindness, normal gonioscopy, (+) provoke test. cataract may be present.
- Deferential DX Primary Open angle glaucoma PACG Infantile glaucoma Other types of glaucoma Final DX: History of steroid use.
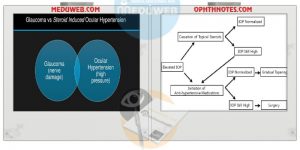
- Management & Treatment Medical stop of corticosteroids or use an alternative agent (less powerful steroid or NSAID) patient’s IOP does not normalize upon cessation of the steroid or in those patients who must continue on corticosteroid medications, use standard antiglaucoma medications ( pilocarpine, beta blocker )
- Management & Treatment(…) Surgical When medical therapy is ineffective or the patient is intolerant of medical therapy, then surgical therapy is indicated. In patients with an open angle and the absence of ocular inflammation, argon laser trabeculoplasty can be attempted. In patients whom both medical and laser therapy have failed , surgical therapy is warranted. Usually, trabeculectomy (guarded filtration procedure), with or without intraoperative antimetabolites, is the primary procedure. In cases of eyes with active neovascularization or inflammation, a glaucoma drainage implant may be used as the primary procedure.