
{kind=link}
Bartholin Cyst:
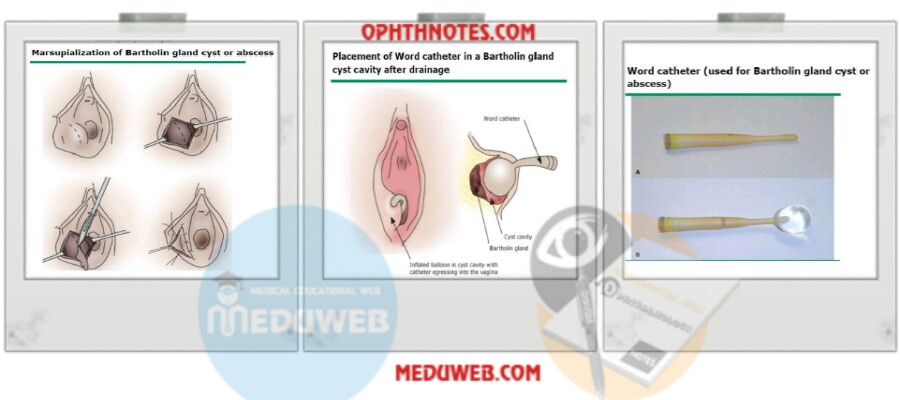
– Cysts that are disfiguring or symptomatic are treated with incision & drainage (I&D) with Word catheter placements (in office) & if recurred after 1-2 times do marsupialization (in operating room).
– No intervention is necessary for asymptomatic Bartholin cysts except for women >40 years, we do I&D to take a biopsy to exclude carcinoma.
Bartholin Abscess:
– The mainstay of treatment is I&D with placement of a Word catheter under local
anesthesia.
– Send a culture for the pus & give antibiotics if positive for gonorrhea or chlamydia or MRSA.
– Start oral antibiotic if suspected complicated infection.
– Start IV antibiotic if systemic infection.
– If abscess recur, I&D with placement of a Word catheter & antibiotics.
– If abscess recur, do marsupialization.
– If abscess recur, do gland excision & send for histopathology to exclude carcinoma.
Bartholin Cyst and Abscess Management Techniques:
– For I&D: a small incision (3-5 mm) is made at or superior to the hymenal ring to prevents obvious vulvar scarring. A small, rather than large, incision ensures that the Word catheter stays in place. The fluid then drains spontaneously or is expressed through gentle pressure. The abscess cavity may be irrigated & suctioned.
– The Word catheter is a balloon-tipped device that is inserted into the cyst/abscess cavity immediately after I&D (see pictures down). The bulb of the catheter is then inflated & left in place for at least 4 weeks to promote formation of an epithelialized tract for drainage of glandular secretions. The end of the catheter is tucked into the vagina to minimize discomfort. When the tract appears well-epithelialized, the balloon is deflated & the catheter is removed in the office.
– Marsupialization refers to a procedure whereby a new ductal orifice is created. This is achieved by incising the cyst/abscess and then everting& suturing the epithelium to the at the edge of the incision. The incision may be either: a single 1.5-2 cm incision, a
cruciate incision or excising a 1-2 cm ellipse of tissue that includes the epithelial surface & the roof of the cyst. The incision is made where the cyst protrudes into the vestibule & just outside of the hymenal ring. The edge of the proximal duct wall is then grasped with fine forceps and everted onto the epithelial surface where it is sutured with interrupted absorbable sutures, thus creating a fenestration for exit of the glandular secretions (see picture down & video in the comments). The cyst/abscess cavity is irrigated; some
clinicians insert a drain or pack for a few days, but this is probably unnecessary.
– Gland excision: In contrast to other methods, excision carries a high risk of
complications, particularly excessive bleeding.
Indications for antibiotics:
●Recurrent Bartholin abscess.
●High risk of complicated infection (such as sepsis), surrounding cellulitis, pregnancy, immunocompromised, DM.
●Culture-positive methicillin-resistant Staphylococcus aureus (MRSA)
●Signs of systemic infection (eg, fever, chills).
Bartholin Cyst and Abscess Management Regimens:
– Trimethoprim-sulfamethoxazole (Sutrim forte; one double-strength tablet twice daily for 7 days) is the first-line agent for patients who are candidates for oral therapy & who are treated as outpatients.
– Alternatives; Amoxicillin-clavulanate (875 mg orally twice daily for 1 week to cover E. coli & Streptococcus species), plus clindamycin (300 mg orally 4 times per day for 1 week to cover Staphylococcal species including community-associated MRSA &Bacteroides).
– The regimen may have to be modified based upon culture results (eg, if chlamydia is present, administer azithromycin 1 gm orally as a single dose.
Management of Bartholin Cyst and Abscess in Pregnant women:
There are no data regarding management of Bartholin cyst/abscess in pregnant women. In our practice, we treat these in the same manner as non-pregnant. One
exception is that we usually do not perform cyst excision during pregnancy or the immediate postpartum period dt.the increased risk of excessive bleeding.