
{kind=link}
 Classification of Diabetic retinopathy
Classification of Diabetic retinopathy
✍️ Mild non-proliferative diabetic retinopathy (NPDR)
![]() ☝️ At least one microaneurysm.
☝️ At least one microaneurysm.
✍️ Moderate non-proliferative diabetic retinopathy (one of the following )
![]() ☝️ intraretinal haemorrhages
☝️ intraretinal haemorrhages
![]() ☝️microaneurysms
☝️microaneurysms
![]() ☝️ cotton-wool spots
☝️ cotton-wool spots
![]() ☝️venous beading
☝️venous beading
![]() ☝️intraretinal microvascular abnormalities (IRMA).
☝️intraretinal microvascular abnormalities (IRMA).
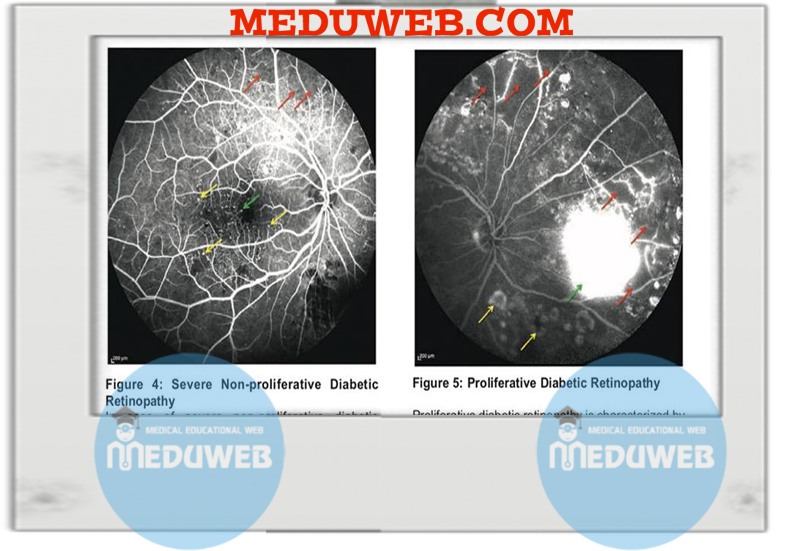
✍️ Severe nonproliferative diabetic retinopathy
![]() ☝️relies on the 4–2-1 rule
☝️relies on the 4–2-1 rule
![]() ☝️ Intraretinal haemorrhages or microaneurysms in 4 quadrants.
☝️ Intraretinal haemorrhages or microaneurysms in 4 quadrants.
![]() ☝️ Venous beading in 2 quadrants.
☝️ Venous beading in 2 quadrants.
![]() ☝️IRMA in 1 quadrant.
☝️IRMA in 1 quadrant.
✍️ Very severe non-proliferative diabetic retinopathy
![]() ☝️at least two of the criteria for severe NPDR.
☝️at least two of the criteria for severe NPDR.
✍️ Non-high risk proliferative diabetic retinopathy
![]() ☝️new vessels on the disc (NVD) or elsewhere (NVE), but criteria not met for high-risk proliferative diabetic retinopathy (PDR) below.
☝️new vessels on the disc (NVD) or elsewhere (NVE), but criteria not met for high-risk proliferative diabetic retinopathy (PDR) below.
✍️ High-risk proliferative diabetic retinopathy: at least one of the following:
![]() ☝️NVD >1/3 disc area.
☝️NVD >1/3 disc area.
![]() ☝️NVD plus vitreous or preretinal haemorrhage.
☝️NVD plus vitreous or preretinal haemorrhage.
![]() ☝️NVE >1/2 disc area plus preretinal or vitreous haemorrhage.
☝️NVE >1/2 disc area plus preretinal or vitreous haemorrhage.
✍️ Advanced proliferative diabetic retinopathy
![]() ☝️tractional retinal detachment.
☝️tractional retinal detachment.
![]() 🛑 High risk DR from from severe NPDR to advanced PDR
🛑 High risk DR from from severe NPDR to advanced PDR
![]() 🛑 Macular exudates or thickening ( maculopathy ) can occur with any severity of retinopathy.
🛑 Macular exudates or thickening ( maculopathy ) can occur with any severity of retinopathy.
Clinically significant macular edema (CSME)
✍️ Definition one of the following
![]() ☝️ Thickening within 500 μm of the macular center
☝️ Thickening within 500 μm of the macular center
![]() ☝️ Hard exudate within 500 μm of the macular center with associated thickening of adjacent retina
☝️ Hard exudate within 500 μm of the macular center with associated thickening of adjacent retina
![]() ☝️ Zone of retinal thickening 1 disc area in size, any part of which is within 1 disc diameter of the macular center
☝️ Zone of retinal thickening 1 disc area in size, any part of which is within 1 disc diameter of the macular center
![]() 🛑 Asymmetric diabetic retinopathy is usually due to carotid disease (on either side)
🛑 Asymmetric diabetic retinopathy is usually due to carotid disease (on either side)
![]() 🛑 Main cause of vision loss in NPDR
🛑 Main cause of vision loss in NPDR
![]() ☝️ macular edema
☝️ macular edema
![]() ☝️ macular ischemia
☝️ macular ischemia
![]() 🛑 Main causes of vision loss in PDR
🛑 Main causes of vision loss in PDR
![]() ☝️ tractional maculopathy
☝️ tractional maculopathy
![]() ☝️ tractional RD (TRD)
☝️ tractional RD (TRD)
![]() ☝️ neovascular glaucoma (NVG)
☝️ neovascular glaucoma (NVG)
![]() ☝️ vitreous hemorrhage (VH)
☝️ vitreous hemorrhage (VH)
![]() 🛑 common diabetic sequelae
🛑 common diabetic sequelae
✍️ Diabetic cataract
![]() ☝️ aldose reductase pathway converts glucose into sorbitol and fructose causing osmotic effect
☝️ aldose reductase pathway converts glucose into sorbitol and fructose causing osmotic effect
![]() ☝️ aldose reductase also converts galactose into galactitol (which causes cataracts in galactosemia)
☝️ aldose reductase also converts galactose into galactitol (which causes cataracts in galactosemia)
✍️ Diabetic iridopathy
![]() ☝️ iris NV
☝️ iris NV
![]() ☝️ lacy vacuolization of iris pigment epithelium in 40%
☝️ lacy vacuolization of iris pigment epithelium in 40%
![]() ☝️ glycogen-filled cysts in iris pigment epithelium
☝️ glycogen-filled cysts in iris pigment epithelium
✍️ Papillitis
![]() ☝️acute disc swelling
☝️acute disc swelling
![]() ☝️ vision usually 20/50
☝️ vision usually 20/50
![]() ☝️ 50% bilateral
☝️ 50% bilateral
![]() ☝️ may have VF defect
☝️ may have VF defect
![]() ☝️ most recover to 20/30
☝️ most recover to 20/30
✍️ Isolated cranial nerve palsies
![]() ☝️ CN 3 ( including pupil- sparing CN 3 palsy)
☝️ CN 3 ( including pupil- sparing CN 3 palsy)
![]() ☝️ CN 4
☝️ CN 4
![]() ☝️ CN 6
☝️ CN 6
✍️ Pupillary abnormalities
![]() ☝️ light-near dissociation
☝️ light-near dissociation
✍️ Fluctuation in refractive error
![]() ☝️ due to osmotic effect on crystalline lens from unstable blood sugar levels
☝️ due to osmotic effect on crystalline lens from unstable blood sugar levels
![]() ☝️ Don’t change glasses power if HBA1c > 7
☝️ Don’t change glasses power if HBA1c > 7
✍️ NVG

Managing diabetic retinopathy
✍️ none/background
![]() ☝️ Discharge to community screening service for annual review
☝️ Discharge to community screening service for annual review
![]() ☝️ if significant systemic disease,
☝️ if significant systemic disease,
consider review at 9–12 monthly by hospital eye service
✍️ Pre-proliferative
![]() ☝️ Observe 4–6-monthly
☝️ Observe 4–6-monthly
![]() ☝️ consider early PRP in select cases
☝️ consider early PRP in select cases
* in single eye patient where first eye lost from PDR
* prior to cataract surgery
✍️ Proliferative active
![]() ☝️PRP 1 or 2 sessions (≥1,000 × 200 to 500 microns × 0.1s) this should occur on the same day or within 2wk
☝️PRP 1 or 2 sessions (≥1,000 × 200 to 500 microns × 0.1s) this should occur on the same day or within 2wk
![]() ☝️ In young patients with type 1 diabetes, PRP should be delivered over 3–4 sessions, as increased risk of macular oedema post-PRP if excess burns applied in single session
☝️ In young patients with type 1 diabetes, PRP should be delivered over 3–4 sessions, as increased risk of macular oedema post-PRP if excess burns applied in single session
![]() ☝️ anti-VEGF therapies is optional
☝️ anti-VEGF therapies is optional
✍️ Proliferative (regressed)
![]() ☝️ Observe 4 to 6 monthly
☝️ Observe 4 to 6 monthly
![]() ☝️ signs of decreased neovascularization activity
☝️ signs of decreased neovascularization activity
* regression of vessels ± fibrosis
* resolution of retinal haemorrhages
* decreases in retinal vessel dilatation and tortuosity
✍️ Proliferative with coexisting DMO
![]() ☝️ For high-risk cases, consider combined macular laser and PRP (with completion of PRP over three sessions, rather than 1 to 2).
☝️ For high-risk cases, consider combined macular laser and PRP (with completion of PRP over three sessions, rather than 1 to 2).
![]() ☝️ For low-risk cases, it may be possible to perform macular laser initially, with PRP at subsequent follow-up.
☝️ For low-risk cases, it may be possible to perform macular laser initially, with PRP at subsequent follow-up.
![]() ☝️ Anti-VEGF therapies may be of particular use
☝️ Anti-VEGF therapies may be of particular use
Managing of diabetic maculopathy
✍️ Focal leakage
![]() ☝️ Focal laser photocoagulation (n × 50–100 microns × 0.08–0.1s)
☝️ Focal laser photocoagulation (n × 50–100 microns × 0.08–0.1s)
![]() ☝️ review at 3 to 4 months
☝️ review at 3 to 4 months
✍️ Diffuse leakage
![]() ☝️ grid laser photocoagulation (n × 100–200 microns × 0.1 s)
☝️ grid laser photocoagulation (n × 100–200 microns × 0.1 s)
![]() ☝️ review at 3 to 4 months
☝️ review at 3 to 4 months
![]() ☝️ Ischaemic
☝️ Ischaemic
![]() ☝️ FFA to confirm diagnosis
☝️ FFA to confirm diagnosis
![]() ☝️ observation may be appropriate
☝️ observation may be appropriate
* significant ischaemia
* no response to previous laser
✍️ Persistent maculopathy
![]() ☝️Anti-VEGF therapies
☝️Anti-VEGF therapies
* ranibizumab approved for cases with central retinal thickness >400 microns
* intravitreal Kenacort in pseudophakic eyes
![]() ☝️ vitrectomy if vitreomacular traction or persistent VH
☝️ vitrectomy if vitreomacular traction or persistent VH
✍️ Rubeosis
![]() ☝️ clear media urgent PRP
☝️ clear media urgent PRP
![]() ☝️ media opacity use anti-VEGF therapies
☝️ media opacity use anti-VEGF therapies
![]() ☝️ monitoring NVG
☝️ monitoring NVG
![]() 🛑 indicators for poor prognosis in CSME after laser photocoagulation
🛑 indicators for poor prognosis in CSME after laser photocoagulation
![]() ☝️ Extensive macular capillary non-perfusion (ischemic maculopathy)
☝️ Extensive macular capillary non-perfusion (ischemic maculopathy)
![]() ☝️Diffuse disease
☝️Diffuse disease
![]() ☝️Cystoid macular edema (longstanding )
☝️Cystoid macular edema (longstanding )
![]() ☝️Lamellar macular hole.
☝️Lamellar macular hole.